
CHRONIC PAIN
Chronic pain is usually defined as acute pain that has lasted for more than six months. More expansively, any problematic pain that lasts more than the typical healing period has become a "chronic pain".
If six months has elapsed since the date of injury and a continuation of the pain, it is reasonable to assume that the injury will cause problematic chronic pain and structural issues indefinitely. At this point, the typical medical strategies shift to "Pain Management" as opposed to pain eradication.
Chronic pain eradication requires a strategy beyond standard a "Pain Management" medical diagnosis, prescription, and treatment.
Understanding the primary causes and secondary contributing factors of chronic pain with more precision can yield rational, sequential strategies for treatment.
In suffering a structural injury with any degree of severity, there are certain realities that can accompany the healing process:
- the restriction in range of motion of a limb or joint in comparison to its range prior to the injury.
- nerve damage, nerve pain, and impaired nerve function that may improve slowly and/or never fully heal.
- loss of motor function, structure, articulation, and/or strength in a limb or joint.
Most severe structural injuries experience some level of healing, but very few completely heal to where the body is operating at the same level as before the injury. Partial healing is a fact of nature with significant injuries, i.e. "sharp pains turn into dull aches".
As people recovering from serious structural injuries become more active again, the recurrence of injury is always looming in the areas of the body that continue to feel compromised.
SCAR TISSUE ADHESIONS
Resulting "scar-tissue" adhesions affecting the injured area are the primary culprits for prolonging pain. Muscles, tendons, and ligaments secrete a kind of "glue"/collagen when torn. This "glue" aids in "casting"/supporting the affected areas to provide post-injury structure.
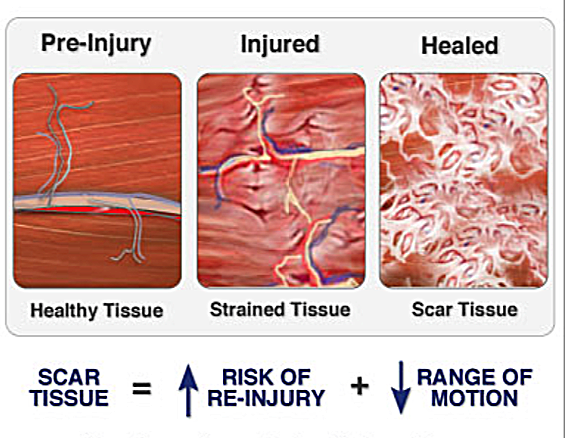 This is the best
image I could find to give a visual of an injury with
scar-tissue formation.
This is the best
image I could find to give a visual of an injury with
scar-tissue formation.The resulting web of scar-tissue adhesions serve to support the injured muscles structurally in basic locomotion. However, they also serve to restrict the range of motion in the affected area through this kind of "binding" as healing progresses...so with support comes restriction.
The collagen protein fibers quite strong, and the spider web structures of scar-tissue collagen in an injured area can severely restrict range of motion by restraining the muscles, tendons, ligaments and nerves in a compromised and painful position.
With respect to athletic movement injuries, there is a high probability that pre-existing scar-tissue adhesions contributed to the latest injury. Areas of the body that have been injured previously are the most prone to re-injury because of the restrictions that these adhesions place on the limb when physical stress increases.
For example, in my own history, a knee injury led to a hip pointer: the scar-tissue above my knee around the femoral nerve pulled so tightly when I was throwing a hard kick (towards the end of a workout...imagine that) that the femoral nerve contracted strongly enough to cause a "hip-pointer" on the same nerve line at the level of the hip.
When overwhelmed by the pain of a hip-pointer, one isn't necessarily reflecting on the fact that the knee caused the situation, especially because the knee is comparatively pain-free while the hip is suffering.
The good news is that these scar-tissue adhesions can be "broken" and "unwoven" correctly through manual manipulation if done by an expert.
To undo existing scar-tissue adhesions in an injured area, a massage therapist must have power, pin-point accuracy, and a superior understanding of the muscle and nerve structures.
In fact, it is possible to break up historical scar-tissue adhesions that existed locally before the current injury, as well as scar tissue adhesions from the current injury, and reset the body to a state much better than before the current injury.
It is possible to rewind "FATHER TIME" with respect to historical, accumulated scar-tissue adhesions: the more of these that are broken up, the further you rewind the clock from the injuries of your body.
PERIPHERAL NERVOUS SYSTEM DYSFUNCTION
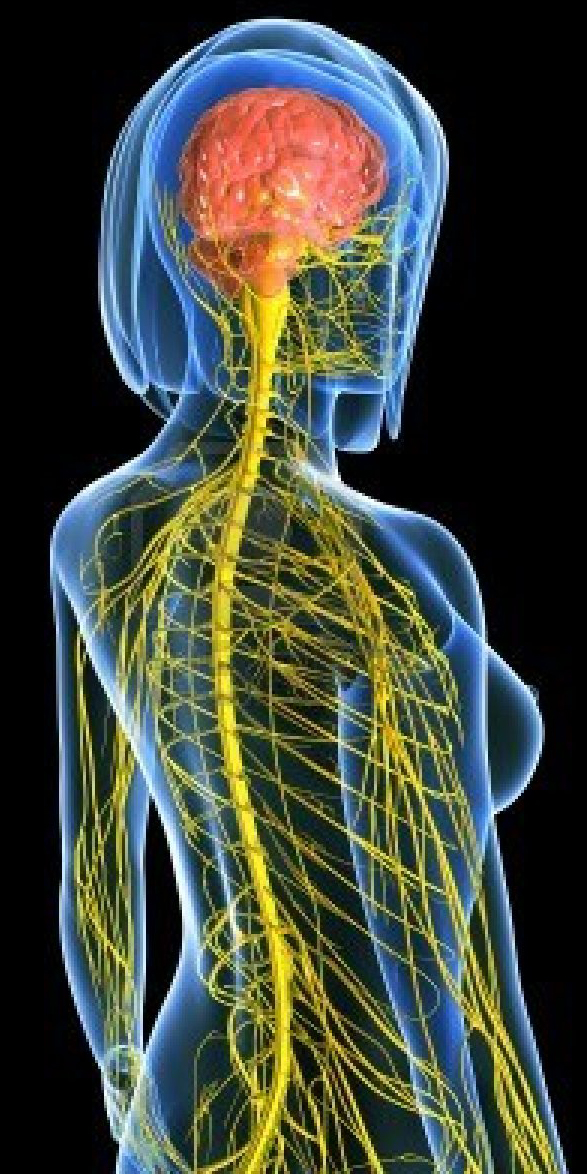 Nervous System: the somatic
peripheral nervous system connects muscles back to the
central nervous and brain.
Nervous System: the somatic
peripheral nervous system connects muscles back to the
central nervous and brain.Currently, too much medical emphasis in the healing process for structural injuries is placed on muscles, tendons, and ligaments. Surgeries are an absolute necessity at times to repair serious injuries to joints, broken bones and the like, but once in "post-op" environment of traditional Western physical therapy, the emphasis shifts disproportionately to these obvious structures.
If repaired correctly and there continues to be chronic pain or reduced motor function, as is the case with many back, knee, and shoulder surgeries, Western physical therapy's spotty track record is due to the fact that the emphasis is so focused on the muscles. Once this level of treatment is exhausted, there is a huge question of where to go from there.
The most overlooked and under-treated structures for success in healing injuries are the somatic peripheral nerves that innervate the muscles in an injured area. To be able to treat these nerve structures correctly is the key to fully eliminating chronic pain and restoring full motor function.
The peripheral nervous system contracts strongly when there is sufficient injury-causing stress placed on the body. Whether in the context of a car accident or athletic movement, when the body braces for or after impact, the nervous system typically contracts dramatically.
Post-injury, these nervous system contractions may release fully, but, more times than not, there is some kind of partial "perma-spasm" operating underneath the surface of reduced muscular function.
This kind of spasming, coupled with the resulting scar-tissue collagen binding around the nerves running through a limb, can trigger a constant pain signal in the brain and further hinder muscle performance. The body's natural electric current in the area is reduced, which means circulation and muscle recruitment are likewise reduced.
A key concept of the entire healing process can be reduced to:
Nerves control muscles==>
Muscles control bones==>
Bones form joints.
Treat and lengthen the nerves innervating the muscles of an injured limb, and the muscles will receive amplified signals for release and healing. If the muscles release on that injured limb, the bones of that limb will house the joints correctly: the joints will be free to release and open to their natural, correct positions.
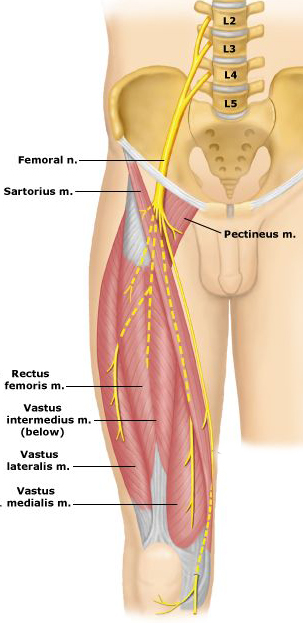 The
Femoral Nerve
The
Femoral NerveFor example, an injury to the femoral nerve above the knee at the level of the hip can so contract the muscles of the quadriceps that they, in turn, tighten the knee joint with a strong, continuous upward pull. This nerve caused muscular stress continues to aggravate the tendons and ligaments of the knee that would otherwise be healing.
Every subsequent shock the femoral nerve now tightens the joint and further stresses the knee structures. How can a meniscus heal when the muscles above it are creating so much pressure that it is grinding against the femur?
I have treated many people with knee issues successfully who thought a surgery was imminent. The continuing sensation of pain at the joint created a false sense of interior damage. My own knee pain, which was a constant for two years, has completed subsided for the last 20 years. During this period, I have trained as hard as I have ever trained...without incident.
Many injured people suffer from this "lumbar vertebrae/lumbar plexus, low back, hip, knee, ankle, and foot pain chain" without ever understanding how the peripheral nervous system is connecting these areas and impacting the situation.
A parallel chain can be found in the cervical vertebrae/brachial plexus, neck, shoulder, elbow, wrist, and hand line. In a typical carpal tunnel case, the cervical vertebrae/brachial plexus damage usually figures to be about 70-90% of the cause. If the therapist is only examining and treating the forearm and wrist, the results will be compromised.
In fact, many of the therapists attempting to treat these kinds of injuries have no idea on how to manipulate the peripheral nervous system successfully along an entire tract of nerve.
Eastern Medicine is specifically designed to heal utilizing the entire nervous system. If one thinks of the nervous system as the "skeleton" of the electric system of the body, a more rational approach for understanding "chi/prana" as the body's animating energy can be formed. The electrical impulses traveling through the nervous system could be likened to the flow of "chi"/energy through the acupuncture channels.
In Eastern Medicine, pain is thought of as resulting from "stagnation" of the body's energy lines or "meridians" in the effected area. With this perspective of somatic peripheral nerve function and electric flow being compromised through injury, there is a congruence between Eastern thought and functional Western anatomy.
In treating the somatic peripheral nerves running from the muscles back to the spinal chord, both scar-tissue adhesions locally and at nerve root sites along the spinal chord can be "unwoven" so that entire limbs release back into a more perfect state. The nervous system electric flow can return to an enhanced state where the pain has subsided and limb function has returned to normal.
The somatic peripheral nerves can be "released" and "reset" through manual manipulation. The technique has to incorporate the exact angles for delivery of pressure to the nerves of each limb respectively in a variety of positions and movement situations.
If this approach is combined with a successful scar-tissue adhesion "cleanse", seemingly devastating injuries and long-term asymmetries can be treated so that there is no further chronic pain or structural compromise.
In fact...
There is no other way to reset the body back to its original state, pre-injury, with respect to scar-tissue adhesions and peripheral nervous system dysfunction other than through expert manual manipulation.